.png)
Why do healthcare costs feel so confusing? Explore the historical decisions that shaped today’s U.S. healthcare pricing system.

the scene
.png "Square, warm‑toned image blending historical medical ledgers and early healthcare documents with soft archival textures, evoking the evolution of healthcare costs over time.")
The Confusion of Healthcare Costs
Before we look back at the “why” behind healthcare costs, let’s put ourselves in a situation many have experienced. Think back to a time when you went to a doctor’s office for a visit. You check in, receive care, and eventually are on your way to continuing your day. A few months pass, and you likely forgot about this appointment, but your healthcare provider and insurance company certainly did not. Because now, you have mail.
You open the letter and discover an unexpected balance due. As frustration sets in, questions quickly follow: “Why do I owe this? What did my insurance pay for?” And perhaps most importantly, “What didn’t it pay for?”
You are not alone in this frustration. In fact, 51% of insured adults report difficulty understanding their own health insurance (Palosky, 2023). This lack of cost clarity did not stem from a single decision, law, or policy. Instead, it developed over time through a series of accumulated choices and differing priorities.
In our first article, we explored how medical providers in colonial Philadelphia were compensated for their services. These transactions often involved trading goods such as textiles, livestock, and bread, as well as exchanging services or labor (Miller & Allen, 2016). During this period, currency was scarce, and healthcare operated within close‑knit communities. This reliance on shared resources fostered trust and flexibility, allowing prices to vary based on what patients could offer and what providers deemed reasonable.
On the surface, this adaptability may sound appealing. However, medical options during this time were limited, and physicians did not undergo the extensive formal education required today. Instead, many were trained through apprenticeships and relied on "traditional" treatments, such as bloodletting, that were later shown to be largely ineffective and, in some cases, harmful (Health Network Group, 2019).
Over the next 150 years, the way healthcare was paid for remained relatively consistent, with a few notable changes as the country industrialized. These included accident policies written by the Franklin Health Assurance Company of Massachusetts in 1850 and the first employer‑sponsored group disability policy introduced by Montgomery Ward & Co. in 1910 (Scofea, 1994). While these programs helped replace lost wages, they did not directly cover the cost of healthcare services.
A more significant shift occurred in 1929 at Baylor Hospital in Dallas, Texas, when the first pre‑paid hospital plan was introduced. Offered to local schoolteachers for 50 cents a month, the plan provided coverage for hospital care, up to 21 days per year, at Baylor Hospital. While this made costs more predictable for patients and helped stabilize hospital revenue, physician services were not included.
As a result, patients remained responsible for many medical expenses. In response, employer groups in industries such as lumber and mining began offering coverage specifically for physician services (Academic Health Plans). These early pre‑paid plans commonly reimbursed hospitals and providers using cost‑based reimbursement. Meaning providers were reimbursed for the reported cost of services, plus an additional percentage intended to support operations (Solace).
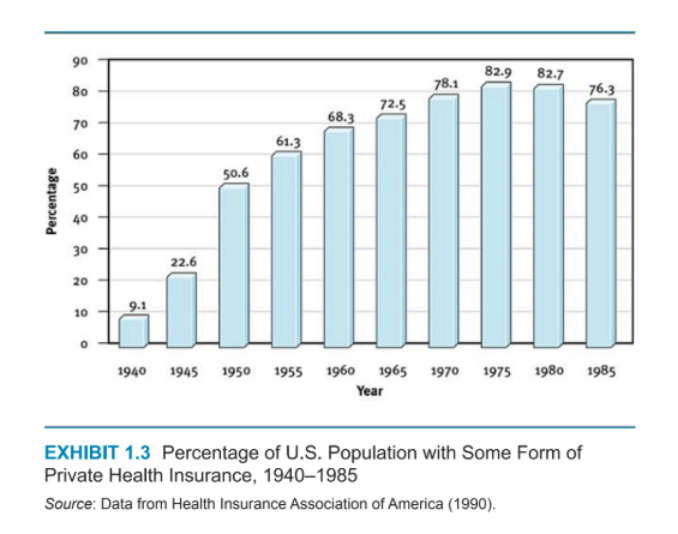
Over time, these pre‑paid models grew in size and complexity and sparked ongoing debate about how healthcare should be paid for. While there were many arguments both for and against these approaches, one thing was clear: participation in private health insurance expanded rapidly. The percentage of the U.S. population enrolled in some form of private health insurance rose from 9.1% in 1940 to 82.9% in 1975 (Morrisey, 2025). This shift reflected changing expectations around how Americans believed healthcare should be financed.
Private health insurance was not the only form of coverage to expand during this time. In 1965, Medicare and Medicaid were established with the passage of the Social Security Amendments, signed into law by President Lyndon B. Johnson (National Archives, 2022). Medicare provided coverage for older adults, while Medicaid focused on individuals and families with limited incomes.
Initially, these programs relied on cost‑based reimbursement models similar to earlier pre‑paid plans. However, as medical technology advanced and healthcare costs increased, this approach became increasingly difficult to sustain. In 1983, Medicare changed how hospitals were paid moving to a fixed payment based on patient diagnosis rather than reported costs.
Private insurers followed suit, developing new payment structures and plan types, including Health Maintenance Organizations (HMOs), Preferred Provider Organizations (PPOs), Point of Service (POS) plans, and later, High‑Deductible Health Plans (HDHPs). While we will explore the differences among these plans in more detail later, the introduction of PPOs marked an important shift by bringing hospital and provider negotiations into the payment process, with the goal of managing costs while maintaining access for employer‑sponsored plans (Morrisey, 2025).
Another major shift occurred with the implementation of the Affordable Care Act (ACA). The ACA aimed to make health insurance more accessible, expand Medicaid eligibility, and support new approaches to care delivery designed to help moderate cost growth (HealthCare.gov, n.d.). The law also prohibited insurers from denying coverage or charging higher premiums based on pre‑existing conditions (HHS, n.d.).
Understanding how we arrived at today’s system helps clarify why healthcare costs can feel confusing and why simple solutions are rare.
The evolution of healthcare payment in the United States reflects a series of historical responses to changing social, economic, and medical needs. From barter systems to employer‑sponsored insurance, government programs, and legislative reform, each solution addressed a challenge of its time, while adding new layers to the system.
Together, these decisions reveal an ongoing effort to balance access, cost, and responsibility in American healthcare and help explain why the system operates as it does today.
Academic Health Plans. (n.d.). A Brief History of Private Insurance in the United States. Grapevine, Texas, United States of America. Retrieved from https://www.ahpcare.com/a-brief-history-of-private-insurance-in-the-united-states/
Assistant Secretary for Public Affairs. (n.d.). Pre-Existing Conditions. U.S. Department of Health and Human Services. Retrieved February 16, 2026, from https://www.hhs.gov/healthcare/about-the-aca/pre-existing-conditions/index.html
Blue Cross Blue Shield. (n.d.). Leading the Way in Health Insurance. Retrieved from https://www.bcbs.com/about-us/blue-cross-history-of-healthcare
Health Network Group Takes a Deep Dive into Healthcare in 1776. (2019, July 3). Retrieved from BioSpace: https://www.biospace.com/health-network-group-takes-a-deep-dive-into-healthcare-in-1776
HealthCare.gov. (n.d.). Affordable Care Act (ACA). Retrieved from HealthCare.gov: https://www.healthcare.gov/glossary/affordable-care-act/
Miller, J., & Allen, E. (2016, April 28). Paying the Doctor in 18th-Century Philadelphia. Library of Congress Blogs. Library of Congress. Retrieved from https://blogs.loc.gov/loc/2016/04/paying-the-doctor-in-18th-century-philadelphia/
Morrisey, M. A. (2025). Health Insurance, Fourth Edition. ACHE Learn. Retrieved from https://books.google.com/books?hl=en&lr=&id=az2gEQAAQBAJ&oi=fnd&pg=PT18&dq=Health+insurance&ots=6WVf3j3rP-&sig=BMHrrKGX8hOrtiXMbbsFNsnOHQw#v=onepage&q&f=false
National Archives. (2022, February 8). Medicare and Medicaid Act (1965). Retrieved from National Archives: https://www.archives.gov/milestone-documents/medicare-and-medicaid-act
Palosky, C. (2023, June 15). KFF Survey Shows Complexity, Red Tape, Denials, Confusion Rivals Affordability as a Problem for Insured Consumers, With Some Saying It Caused Them to Go Without or Delay Care. Retrieved February 9, 2026, from KFF: https://www.kff.org/medicaid/kff-survey-shows-complexity-red-tape-denials-confusion-rivals-affordability-as-a-problem-for-insured-consumers-with-some-saying-it-caused-them-to-go-without-or-delay-care/#:~:text=About%20half%20(51%25)%20of,benefits%20stateme
Scofea, L. A. (1994, March). The development and growth of employer-provided health insurance. Monthly Labor Review, p. 3. Retrieved from https://www.bls.gov/opub/mlr/1994/03/art1full.pdf
Solace. (n.d.). What is Cost-Based Reimbursement? Retrieved February 16, 2026, from https://www.solace.health/glossary/cost-based-reimbursement


.png)

%20(1).png)

Don’t get me wrong, apprenticeships can be valuable learning models, but this raises an important question: would you prefer your physician to complete more than seven years of rigorous education and clinical training, or to rely primarily on a shorter apprenticeship?